How many people will die - no-one
can tell until the final reckoning.
Endless predictions and calculations have
been presented - one of the earliest omissions in daily and weekly totals was the number
dying in care homes, a sector that only came to be accorded proper attention in mid April
2020.
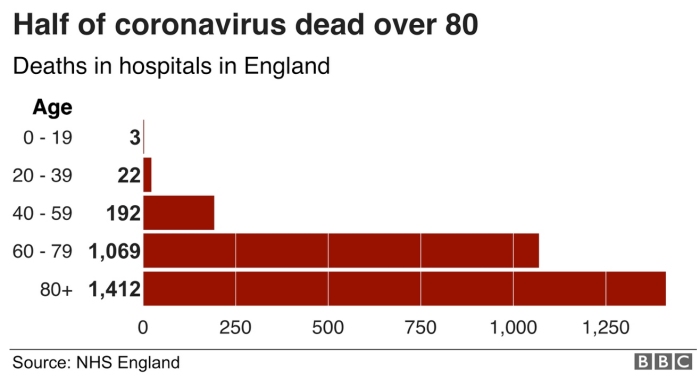
Early data showed most deaths
were in people over 80 - the totals shown here might be far more marked once deaths in
care homes for the elderly were included.
Early government data omitted deaths in care homes. |
 |
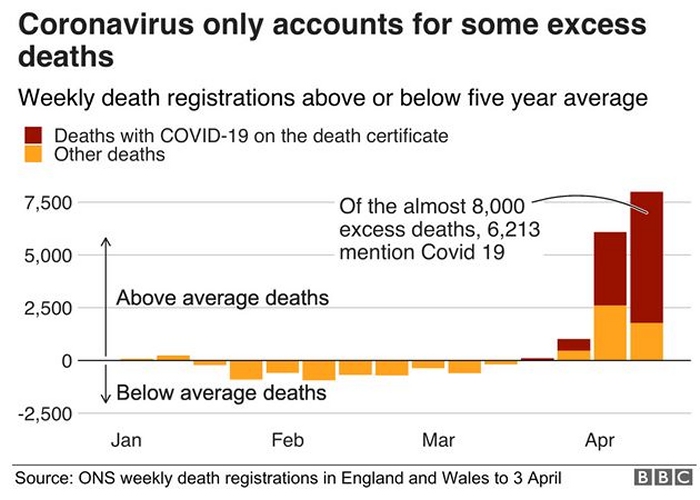
As explained below, this is
the only reliable method of gauging excess deaths - what is put on a death certificate (if
any) can be unreliable where there may be multiple causes (dementia, old age, Covid-19,
etc)
Once other seasonal factors have been accounted for most of the 'excess deaths per month'
may in fact be owing primarily to Covid-19. They may eventually be found to be double
early government estimates.
Many of the 'other deaths' shown here may eventually be found be be primarily related to
Covid-19.
But it is an inexact science, and statisticians may work on the figures for years!
All of the government lock-down was aimed at reducing the peak of deaths to a manageable
level - one that the NHS could cope with in terms of bed spaces and trained staff (and
equipment).
It was never seriously envisaged that tens or maybe hundreds of thousands of covid-related
deaths might be avoided during 2020 and 2021. Only development of a proven vaccine was
thought likely to seriously impact on the total figures. |
 |
Within
forum discussions I summarized my own predictions as follows:
It is probably quite rare for Covid 19 to be the sole cause of death. But that misses a
key point.
In a large number of people who are teetering on the edge of death with one or ten years
still to live (if they are unlucky) Covid 19 can result in a death now rather than in one
or ten years. Any underlying health condition that weakens the body can be a factor -
obesity for example.
At present there is indeed some uncertainty in the statistics of how many people have been
exposed to the virus and how many have died prematurely of Covid 19 outside of hospitals.
The mortality rate is also uncertain - we don't yet know for sure how many people have had
the disease in a mild form and thought nothing of it.
But what is certain is that Covid 19 can produce characteristic symptoms in many people
and some of them die ultimately of pneumonia or immune system overload - both indeed are
symptoms seen before Covid 19 appeared on the scene, because more than one agent can cause
these symptoms. It is also known that some people have the disease and yet do NOT exhibit
the characteristic symptoms, but more those of a cold.
It is already certain that there is a large spike in this characteristic type of death
(pneumonia, and/or immune system overload) with numbers well above the monthly/seasonal
norms that are seen either in hospitals or elsewhere.
When the dust settles, deaths rates in each age band arising from this class of symptoms
can be compared weekly or monthly with historic rates, corrected for factors such as the
severity of the winter.
When I was involved in these things 40+ years ago death rates in the UK were often fairly
stable throughout the year, month by month. In a very severe winter, there was an excess
of up to 30,000, these being people whose death had been brought forward primarily because
of inadequate heating of houses. A few died slipping on the ice of course. So hypothermia
was a prime cause of these early deaths but so was poverty, inadequate food intake, etc.
Few were (I would guess) ever recorded as hypothermia, just as yet another old person
dying often alone at home. We always used to contrast this (occasional) 30,000 excess
during a severe winter in the UK to the 30,000 children who died every DAY in Africa of
starvation (etc). It was back in the days of periodic mass famines. There was no attempt
to log data month by month - only to look back at full year totals.
But it was certain that in a very severe winter there was an excess above the norm in the
UK, no matter how you juggled the figures for that year and no matter to what specific
cause (if any) you ascribed the death. There was little or no corresponding spike in
Sweden - they took winters and insulation of buildings more seriously.
So ultimately, we will get statistics on the excess numbers of deaths with the Covid class
of symptoms, and these will be the Covid-related deaths as an excess above the norm, as
closely as anyone is ever going to know. More may be added that didn't have the most
severe Covid symptoms if a residual bump in the numbers needs to be accounted for.
But all of this must await statistics applied to probably a years' worth of data.
It is semantics to argue whether a death was purely owing to Covid 19 or whether Covid 19
was a contributory factor - 10% or 90% responsible.
Without Covid 19 there would have been no excess over the norms that couldn't be accounted
for by other factors - a bad year of flu for example.
The only real baseline data for now is that in the early weeks of the pandemic hospitals
in the UK were being almost overwhelmed by patients with Covid symptoms. This provides no
more than a minimum estimate of the final numbers.
As of 15 April 2020 however, daily numbers
of deaths seemed to be declining and it was postulated that the new 'Nightingale'
hospitals might not be much used - if only because sufficient numbers of trained staff
were not available?
The biggest field hospital, NHS
Nightingale in London, has already opened.
It has space for 4,000 patients but has taken only a few dozen so far.
Meanwhile, the facility in Birmingham has yet to take in any patients, while the site
planned in north-east England may not now be needed.
Martin Wilson, the chief operating officer for Newcastle Hospitals NHS Foundation Trust,
which is overseeing the Washington project, said: "I don't think we will need to
open.
"If we do, we will be ready."
With these sorts of statements, total lock-down was not envisaged to last much longer. The
economic disruption was simply too great. Lockdown
was only ever primarily to flatten a large spike of cases at a time the NHS was almost
wholly unprepared.
0. Index page.
1. Wet markets, abuses of wildlife, organised crime and the origins
of the virus.
2. Folk dancing and the importance of other 'super-spreader' events -
experience overseas.
3. Scientists, government scientists, and criticisms of government
policy in the UK.
4. How many people will die - no-one can tell until the final
reckoning.
5. Policing of lockdown in the UK - the need for police reform
(starting at the top?).
6. Religious nutcases and despotic governments (often the same
people!)
7. Economics vs. Health - the lockdown cure being worse than the
disease?
8. Ventilators and cures.
9. Shaggy dog stories - and wash your hands.
10. Reserved.
Home page of website